
I recently facilitated a workshop on Polarity Management for a group of surgeons and doctors, who found it extremely beneficial. I had a “before and after” experience when I learned the model – after you see it, you think, “This is so obvious; how did I not know about this model?” In the workshop, we used the tool to discuss the polarity of focus on Cost AND focus on Quality, in which people identify the upsides and the downsides of both poles. The reason this is AND rather than “versus”, is that in a polarity both poles are interdependent and necessary to the system. You can’t get rid of a focus on cost, just like you can’t get rid of concern for quality – you need both to make the system work.
The discussion helped surface several other polarities that happen in their hospitals, and uncovered assumptions that some staff have. For example, one assumption is that “anybody going after quality is blind to cost”. Something else that goes unstated is our interpretation of “quality” – how each of us defines it, and how we as a group define it – another necessary conversation. Each case calls for a facilitated discussion in which there is collective “sense-making”. That means that people share their interpretations and surface their assumptions, so that the group comes to an agreement about the definition of terms.
The workshop also helped identify some discussions that are calling to be had in health systems, especially in light of the Affordable Care Act (ACA). For example, one participant articulated this important question: “How do we set different measurement standards to help us resolve this polarity?” Some participants commented that many doctors are anxious about how the ACA will affect patient care, and their income. Others question physicians’ motivation for choosing medicine, which for some/many seems to have changed over the years, from initial idealism to a focus on money. So you can see the value of the conversation that went beyond the initial polarity.
Lastly, the piece that emerged for me as a facilitator is my interest in providing a safe space for health care providers to talk about their fears and concerns. Using this model helps depersonalize conflict or tension of people pulling in different directions. When you help people see the entire system, the “both/and” of the poles, they gain understanding for the competing commitments of different functions in the organization. It’s never either/or; people have the ability to hold two concerns at the same time – they can attend to the need for both cost and quality, for example.
Where can you use this model in your organization?
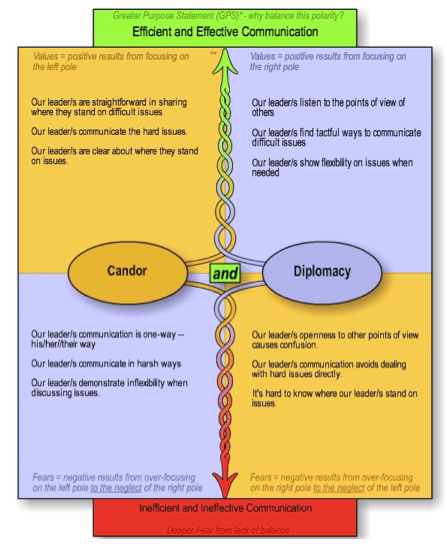
image credit: http://bertparlee.com/training/polarity-management/
Discover more from TRANSFORMATIVE COACHING
Subscribe to get the latest posts sent to your email.

Abby
Thanks for this post. I have also recently discovered polarity management from the work of Barry Johnson and find it very useful. It has made me rethink an issue for physicians that is called by some shifting from an autonomous/independent model of work to a team/interdependent model. Actually it is a polarity –after all, we would not want physicians to become entirely interdependent–patients need individualized decisions as much as they need care according to guidelines assured by team work.
In making a safe place, I also have come to seeing this as crucial. I usually present some norms up front usually tailored to the group unless there is time to create them ourselves (usually not as I am asked to come to work on more specific leadership/team/change topics). Confidentiality is important–particularly how you talk about situations at work. In so many words, talking about suspending certainty and judgment, a brief intro to the ladder of inference. It varies.
What do you think? If we do not create the kind of dialogue in trainings that are needed in the workplace then what is the use/
Thanks again for the post
Neil